


-
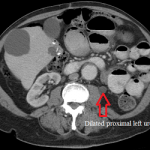
- Axial CT scan of the abdomen before left ureteral stenting showing dilated left ureter.
-
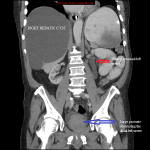
- Coronal CT abdomen and pelvis showing dilated upper left ureter and a large prostate.
-
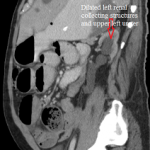
- Sagittal CT abdomen and pelvis showing dilated left ureter and calyces
-

- Lateral fluoroscope early in left ureteral stenting showing dilated left ureter and renal pelvis.
-

- Frontal fluoroscope after left ureteral stenting and rescue left nephrostomy catheter.
-
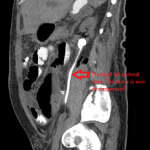
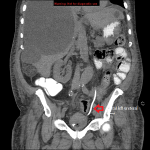
- Sagittal CT abdomen and pelvis after left ureteral insertion showing a decompressed collecting system
-
- Coronal CT abdomen and pelvis showing the distal end of the left ureteral stent in the urinary bladder.
These images illustrate the benefit of ureteral stenting. They are of a male patient with benign prostatic hypertrophy, who recently underwent surgical resection of a colonic malignancy. His imaging workup uncovered left hydronephrosis caused by a retroperitonal mass encasing his distal left ureter. It was not possible stent the ureter from a urethral approach, so he was referred to the interventional radiology service.
Using ultrasound, a needle was inserted into a dilated mid-pole calyx, and an antegrade pyelogram obtained through a sheath inserted to secure the access confirmed marked dilation of the left ureter and the collecting structures of the left kidney. Ureteral stent was deployed over a guidewire passed across the distal ureteral stricture into the urinary bladder and its proximal and distal pigtail loops reformed in the bladder and the left renal pelvis, respectively. A capped rescue nephrostomy catheter was left in the renal pelvis, but was removed later, when the ureteral stent proved sufficient in decompressing the left urinary collecting system.
As I discussed elsewhere, it is important that an obstructed renal collecting system be relieved or the urine accumulated above it and under pressure be drained as soon as possible to avoid renal damage and infection. Optimal relief of such obstruction is with an internal ureteral stent placed through the urethra by a urologist. But when this is infeasible, the stent can be placed antegradely from the back and through the kidney. When successful, a rescue nephrostomy catheter may be left in place, capped, until it is certain that the stent is working well – unless there is no reason to worry about the stent functioning well. The nephrostomy catheter may be removed in 24 hours – 48 hours, barring any contraindications.