What is percutaneous biopsy?
Per means ‘through’ in Latin, ‘cutaneous’ derives from cutis, which is Latin for skin. Bio- is a combining form from the Greek word bios, which means life and opsis is Greek for vision. Percutaneous biopsy then, is the removal of living tissue through the skin, usually with a needle. Tissue can be taken from any organ for analysis and the procedure is frequently an outpatient one. By comparison, in open biopsy a tissue or organ is laid bare, and the operator, under direct view removes a portion or all of an abnormality; removing a part of abnormal tissue is called incisional biopsy, while removing the entire abnormality is excisional biopsy. In both, because of their complexities, the patient is sedated deeply and may even receive general anesthesia.
How is percutaneous biopsy done?
There may or may not be arrangements for you to stay in the hospital or clinic for observation after percutaneous biopsy. This is safe and allows your care provider to detect any complication(s) early and manage them. This aspect of care varies with physicians, a patient’s overall health and the complexity of the biopsy process. You will, quite likely, be asked not to take anything by mouth starting the midnight of the day of your procedure. This allows your physician to expeditiously administer conscious sedation to you should there be need to do so during your biopsy. The procedure is, however, relatively simple and safe and most operators do it with only local anesthesia, allowing the patient early discharge. You may also be asked or have been advised to cease taking such medications as Warfarin (Coumadin), Aspirin and Ibuprofen since these “thin” the blood, raising your chance of bleeding after the biopsy.
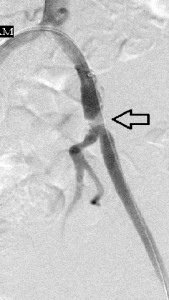
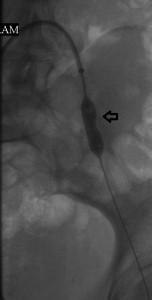
Several decades ago percutaneous biopsies were done blindly, meaning that operators were guided by a sound knowledge of anatomy of the body when biopsying deep body organs; it was and still is easy to biopsy palpable lesions because they are superficial and easily accessible. Blind biopsies in those days were generally done when diffuse involvement of an organ seemed likely, not when there was a nonpalpable focal lesion like a tumor; such would need an open biopsy (excisional or incisional). Today, because of technological advances in medicine, most percutaneous biopsies are done with guidance from imaging modalities like fluoroscopy, ultrasound, CT scan and magnetic resonance imaging (MRI), which eliminates guess work from the procedures, making them safer. You will be asked to lie down, the site of disease reviewed again with an imaging modality, and an appropriate skin entry point selected, cleansed with antiseptic material, and anesthetized. The operator will then make a small nick in the skin with a surgical blade and, through it advance a needle of appropriate size and length, into the numbed track down to the area of interest and remove a few bites of the tissue. He will remove the needle and hold pressure over the biopsy site to arrest mild bleeding that may occur.
How do I prepare for percutaneous biopsy?
First, you or a designee must ask of and receive from your care provider an account of the merits and demerits of this procedure and its alternatives. When you have done this, you must endorse the procedure by signing a document called a consent form. You will inform your physician of and stop taking any of the medicines mentioned above that place you at risk for bleeding.
Who needs percutaneous biopsy?
1. Anyone who has a lesion or disease whose diagnosis is unknown despite other investigations.
2. Anyone with an established disease whose effect on an organ requires monitoring through periodic microscopic reviews of tissue from the organ. For example, patients with hepatitis C virus infection of the liver need be monitored to know when the infection requires treatment.
3. Anyone with a symptom or sign that suggests disease of a specific organ that demands characterization and staging scheme. For example, patients who spill protein in their urine in whom the nature of the underlying kidney disease is best framed by microscopic review of renal tissue.
4. Any other reason(s) your physician may explain to you.
What are contraindications to percutaneous biopsy?
Contraindications are conditions you may have that will make percutaneous biopsy risky for you. You must let your healthcare provider know of them before embarking on this procedure. They include:
1. Uncorrectable coagulopathy (this means ‘thinning’ of your blood which will make you bleed too much).
2. No safe access route.