


History
This was a young female victim of a fatal motor vehicle accident.
Radiologic findings
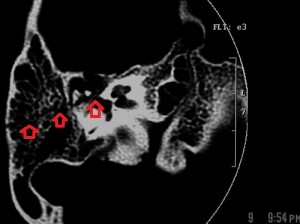
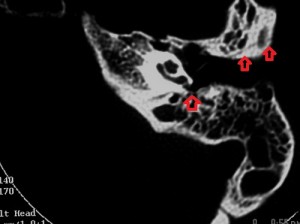
Images A and B are bone-window axial sections of the petrous portions of the right and left temporal bones taken at slightly different levels. Both show longitudinal fractures of the petrous pyramids with slightly different orientations (see the arrows). In addition, there is a fracture line through the anterior right basi-occiput, arrowed on image B.
On the right, the fracture line extends into the right middle ear, across the tegmen tympani and into the middle cranial fossa while on the left it stops at the external auditory meatus. The right ossicular chain is dislocated (incudostapedial joint) but the left chain and the right and left otic capsules are preserved. There is effluent in the right mesotympanum, the reason for a right ottorhea at presentation. There is no fluid in the left middle and external ear. Although the images are not included, there are no injuries to the internal auditory canals
Radiologic diagnosis
1. Longitudinal fractures of the right and left petrous pyramids with right ossicular chain dislocation.
2. Fracture of the anterior basi-occiput.
Discussion
This patient died from other severe body injuries including at least two variants of injury to the skull base – petrous pyramidal fracture and fracture of the basi-occiput. I will dwell on the pyramidal fractures.
Fractures of the petrous pyramids are one of the most common fractures of the base of the skull (the others are fractures of the sphenoid bone, the orbital roof and the basi-occiput).
Petrous pyramidal fractures are due to lateral, frontal or occipital forces to the head and may be longitudinal (parallel to the long axis of the petrous pyramid) or vertical (perpendicular to its long axis). Although the longitudinal pattern is thought commoner (80%), the majority of the injuries are mixed.
Typically inflicted by a tempo-parietal blow, the longitudinal fracture (as in this case) begins from the squamous portion of the temporal bone and the mastoid, travels through the external meatus, passing medially to the tegmen tympani. The middle ear is involved, along with ossicles in some cases; the CT images show opaque mastoid air cells, fluid in the mesotympanum and ossicular fracture or dislocation.
Clinically, there is bleeding from the external meatus, conductive hearing loss, and leakage of CSF from the ear or the mouth (via the Eustachian tube). When the fracture line extends medially, it may either be deflected by the bony labyrinth (which is relatively resistant to fracture), or traverse it, resulting in facial nerve weakness (due to edema), with a favorable prognosis, as well as variable degrees of deafness and vestibular impairment. If there is a fracture of the labyrinth, pneumolabyrinth may occur. When the fracture line travels close to but spares the bony labyrinth, the seventh and eighth cranial nerves may suffer temporary concussional effects (sensorineural deafness, dizziness, balancing problems).
Pure transverse fractures of the petrous pyramid are less common (20% of the fractures) and result from either occipital or frontal forces to the skull. The fracture line travels perpendicular to the long axis of the pyramid. It commonly extends forwards from the jugular fossa or foramen magnum across the temporal bone either through the bony labyrinth or more medially through the internal auditory canal, and severe or complete sensorineural deafness with vestibular paralysis is a common feature. In such patients cochlear implantation may be attempted.
Fractures of the base of the skull may present in various ways depending on the pattern of injuries. Peri-orbital ecchymosis, the raccoon eye, is due to a fracture of the orbital floor; CSF rhinorhea is due to a fracture of the floor of the anterior cranial fossa or may be due to a fracture of the body of the sphenoid bone. Blood or CSF leakage through the mouth (via the Eustachian tube) or the external auditory meatus suggests injury to the floor of the middle cranial fossa (tegmen tympani). William Henry Battle, a British surgeon, described as a sign of basilar skull fracture, skin discoloration in the line of the posterior auricular artery which first appears near the tip of the mastoid process.
There may be conductive hearing impairment due to dislocation or fracture of the middle ear ossicles (these may occur with or without petrous pyramidal fractures) or sensorineural hearing loss due to injury to the inner ear hearing structures or the eighth cranial nerve. The face may droop because of injury to the facial nerve (temporary or permanent) while vestibular injury causes dizziness, vertigo, nausea or vomiting. When your suspicion is aroused, investigate the patient with CT, a good imaging modality for this purpose, to confirm and explore the extent of the likely injuries.
References
1. Yeakley JW. Temporal bone fractures. Curr Probl Diagn Radiol. 1999 May-Jun;28(3):65-98.
2. Hasso AN, Ledington JA. Traumatic injuries of the temporal bone. Otolaryngol Clin North Am. 1988 May;21(2):295-316.
3. Samii M, Tatagiba M. Skull base trauma: diagnosis and management. Neurol Res. 2002 Mar;24(2):147-56. Review.