Smoking, dyslipidemias (disorders of lipids such as hypercholesterolemia), hypertension, and diabetes, individually and severally, may narrow or occlude arteries in all parts of the body.
Amongst arteries that may suffer are the ones that carry blood from the abdominal aorta (the large artery that carries blood from the heart across the abdomen towards the lower limbs), through the pelvis (the waist area), into the lower limbs, called the iliac arteries. If the narrowing of the vessel lumen is significant or the occlusion total, symptoms like claudication (pain during ambulation), paraesthesia, numbness, and erectile dysfunction may develop and bring a patient to medical attention.
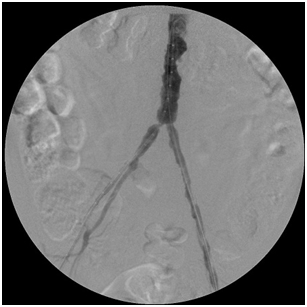
The images below illustrate such a problem. This patient in addition to having irregular chunks of calcium narrow his aorta has significant narrowing of the origins of his common iliac arteries (ostial stenosis), which along with the narrowings above and below them diminished the amount of blood reaching the patient’s feet from the aorta, causing symptoms.
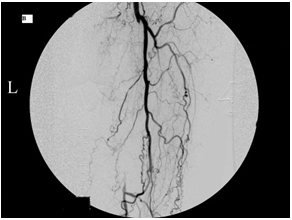
By simultaneously deploying a stent across each common iliac ostial narrowing, I corrected the problem, delivering more blood into the patient’s feet. The first image shows the narrowings before the stents were deployed; the second image displays the process of stent deployment; the third image was taken after I landed the stents.