


One of the causes of infertility in women is obstruction of the fallopian tubes, the two trumpet-like canals that extend from the corners of the uterine fundus towards the ovaries. They conduct eggs released by the ovaries towards the inner chamber of the uterus called the endometrial cavity and may become occluded by disease, typically sexually transmitted disease. More commonly, however, obstruction of the fallopian tube at its cornu (the attachment of the tube to the uterus) is caused by refluxed menstrual debris, not pelvic inflammatory disease. Tubal occlusion from whatever cause impedes the arrival of eggs from the ovaries to the endometrial cavity causing infertility.
The location and type of tubal obstruction vary: obstructions can occur close to or away from the uterine cavity and may be partial or total. Interventional radiologists can reopen fallopian tubal obstructions through a woman’s cervix by a procedure called transcervical recanalization of the fallopian tube. The closer fallopian obstruction is to the uterine cavity, the more likely transcervical recanalization will be successful; more distal obstructions are less reparable by this technique.
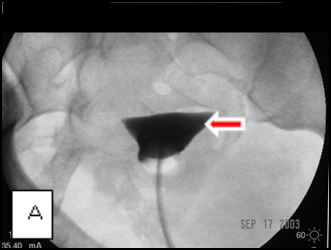
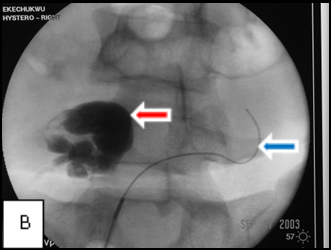
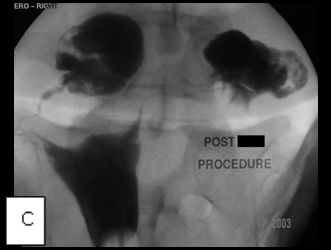
Images A, B, and C belong to a young woman who was referred to me for hysterosalpingography because of infertility and was shown at the examination to have bilateral cornual occlusion of the fallopian tubes. Image A shows contrast opacifying her endometrial cavity (red arrow), but not the fallopian tubes due to bilateral cornual occlusions. In image B, I have reopened the right cornual occlusion, filling a large right hydrosalpinx with radiocontrast (red arrow), and have a guide wire in the left fallopian tube (blue arrow), which implies relief of the obstruction. Image C, the final image, shows that both cornual occlusions are relieved, but there are bilateral large hydrosalpinges because of fimbrial adhesions, proven by the absence of contrast spill into the peritoneal cavity.