


History
This is a 20-year old female who visited the emergency department because of pain in the left lower quadrant of her abdomen. She had no significant past medical problems, but on examination had an excessive amount of hair on her lips, chest, and lower belly. Her pubic hair, though also excessive, was feminine in its distribution. While in the emergency department she had contrast-enhanced CT scan of her abdomen and pelvis, but had no other imaging studies. Measurements of her testosterone while on admission were normal. Later, she underwent open laparotomy and had her abdominal mass removed.
Radiologic findings
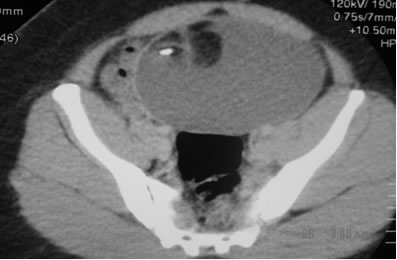
This is a single axial section through the patient’s false pelvis showing a midline, thin-walled (1mm), complex mass. The mass measures 12cm x 13cm x 13cm and at its 10 to 12 o’clock position is a heterogeneous mass of tissue (Rokitansky protuberance, dermoid plug) comprising a high-density rectangular structure (coarse calcification, mal-formed tooth), and lobules of tissue isodense to subcutaneous fat (fat). The preponderance of the mass, however, is hypodense to enhanced muscle but slightly hyperdense to noncontrast urine (not shown); it is fatty debris. The mass is anterior to the rectum, straddles the pelvis and displaces the small bowel to the sides. The ovaries are not discernible. The appearance of the mass is pathognomonic for a mature teratoma.
Differential radiologic diagnosis
There is no differential diagnosis. The radiologic features of the lesion are pathognomonic for benign cystic teratoma of the ovary.
Gross pathologic findings
A large mass which on sectioning revealed:
1. Cheesy liquid debris.
2. A solitary tooth.
3. Thick golden-yellow congealed fatty tissue.
4. A loch of hair.
Please see below.

Final pathologic diagnosis
Mature (Benign) Cystic Teratoma.
Discussion
Teratomas (teratos, Greek for monster) are congenital tumors of derivatives of all three germ layers. They arise from pluripotent embryonal cells and occur in the ovaries, testes, mediastinum, retroperitoneum, and the sacrococcygeal region, in order of decreasing frequency. The location of the tumor in our case suggests that it is ovarian in origin; presacral or retroperitoneal origins are less likely alternatives.
Teratomas are the most common tumors of the ovary in children and adolescents although they may present at any age in life. They may be mature (cystic) or immature (solid, a.k.a embryonal) and carry a 0.25-1.5% risk of malignant degeneration, representing 1% of malignant ovarian tumors. The risk of malignant degeneration is predicted by the presence of neuroectodermal remnants, which the present case lacks.
Two-thirds (67%) of the cases present as an abdominal mass (as in this case) and 10% – 15% are bilateral. Other modes of presentation include abdominal pain (our case), ovarian torsion, nausea, vomiting and, rarely, ascites. There may be rare association with hyperprolactinemia, hemolytic anemia, hyperthyroidism (struma ovarii) or Mayer-Rokitansky-Kuster-Hauser syndrome. The latter consists of a lack of mullerian development, congenital absence of the vagina and rudimentary uterus (typically bicornuate remnants), with normal uterine tubes, ovaries, secondary female sex characteristics and normal growth. There was mention to me by one of the patient’s physicians that she had a small uterus and was hirsute. I doubt that we can invoke Mayer-Rokitansky-Kuster-Hauser syndrome in this case because of the absence of the other features and I doubt that her alleged hirsutism has any relationship to the teratoma. She recuperated well from her surgery and went home in good condition.
References
1. Friedman AC, Pyatt RS, Hartman DS et al 1982. CT of benign cystic teratomas. AJR 138: 659-665.
2. Buy JN et al. Cystic Teratoma of the ovary: CT detection; Radiology 171: 699-701. 1989
3. Kallenberg GA et al. Ectopic hyperprolactinemia resulting from an ovarian teratoma: JAMA, 263: 2472-2474.